Evidence-based Practice (EBP)
")
Evidence-based Practice (EBP) represents a powerful philosophical and practical shift in how professionals approach their work, moving away from tradition, conjecture or purely personal preference. It is fundamentally a disciplined commitment to making decisions through the conscientious and judicious use of the best contemporary research evidence, coupled with the practitioner's developed professional experience, while always considering the unique values, circumstances and preferences of those being served. This tripartite framework is not simply about consulting scientific papers; it demands a critical, skeptical approach to all knowledge sources, ensuring that actions taken are supported by robust, verifiable data, leading to higher accountability and more effective results across various disciplines, from healthcare to management and education
Who coined the term Evidence-Based Medicine?
Dr. Gordon Guyatt, working with colleagues including Dr. David Sackett at McMaster University in Canada, coined and popularized the term in the early 1990s.
What are the three core components of EBP?
EBP integrates external scientific evidence, professional expertise and experience, and client values and preferences. All three components are considered equally essential.
What sits at the top of the evidence hierarchy?
Systematic reviews and meta-analyses occupy the apex, as they synthesize findings from multiple high-quality studies and provide the most comprehensive, least biased estimate of an effect.
How does EBP differ from simply following research findings?
EBP requires practitioners to filter scientific evidence through professional judgment and individual client circumstances. A research-supported intervention may still be inappropriate if it conflicts with a client's values, context, or practical constraints.
In which fields is EBP applied beyond medicine?
By the late 1990s and early 2000s, EBP principles had migrated into nursing, psychology, education, public policy, and management, among other disciplines.
Origin Story
While the systematic approach to using empirical data to guide decisions has roots stretching back centuries in fields like medicine (think of Florence Nightingale's data-driven sanitation reforms), the modern formalized framework of Evidence-based Practice emerged and gained prominence within clinical medicine. The term "Evidence-Based Medicine" (EBM) was notably coined and popularized in the early 1990s by a group of internal medicine specialists and epidemiologists at McMaster University in Canada
Central to this pioneering group was Dr. Gordon Guyatt, who is often credited with first using the phrase in its contemporary context. Guyatt and his colleagues, including Dr. David Sackett, a physician-scientist, set out to develop a new pedagogical approach for teaching clinical practice. They recognized a significant gap: medical training often relied too heavily on anecdotal experience and expert opinion, which could be outdated or inconsistent. Their goal was to instill in trainees the necessary skills to actively search, critically appraise and apply the scientific literature to individual patient care decisions
Dr. David Sackett became the most prominent evangelist for the movement. Sackett defined EBM not as "cookbook medicine" but as:
the conscientious, explicit and judicious use of current best evidence in making decisions about the care of individual patients
His efforts, alongside the work of the Evidence-Based Medicine Working Group at McMaster and eventually the establishment of the Cochrane Collaboration (which systematically reviews randomized controlled trials), provided the methodological infrastructure needed for EBP to flourish
The underlying philosophy was quickly adopted and adapted by other disciplines. By the late 1990s and early 2000s, the principles were migrating into fields like nursing, psychology, education and public policy, leading to the broader designation: Evidence-based Practice (EBP). Though the original authors worked within medicine, their contribution was not just a medical technique but a rigorous, transferable epistemological framework—a standardized way of knowing—that champions empirical rigor over intuition in complex professional domains. The legacy of Guyatt and Sackett lies in creating a universally recognized standard for decision-making that demands continuous learning and a humble acknowledgment of the limits of personal expertise without scientific backing.
The core mechanism of Evidence-based Practice is best understood as a cyclical and integrated model, rather than a linear sequence. It demands the integration of three distinct, yet equally essential, components, symbolized as the three interlocking rings of a rigorous professional commitment.
Component I
External Scientific Evidence
This element constitutes the systematic findings derived from high-quality, reproducible research. It is the bedrock of objective data, designed to test hypotheses and establish generalizable truths about what works and why. Practitioners must develop a sophisticated understanding of the hierarchy of evidence, which serves as a guiding map for assessing the validity and reliability of different study designs.
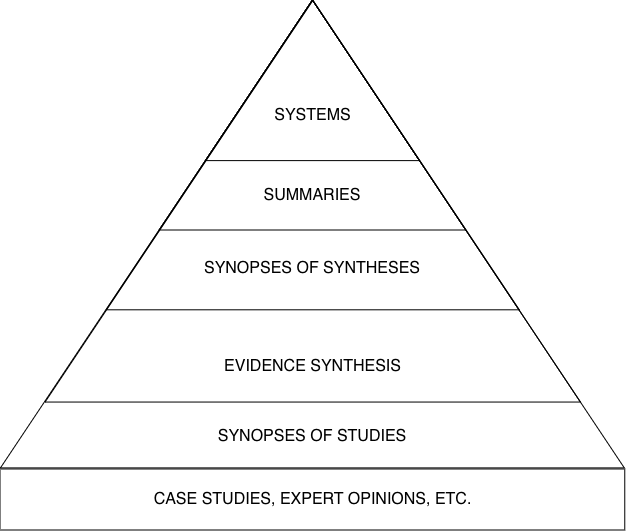
The structure of the hierarchy reflects the degree to which a study design can minimize bias and confounding factors, thereby increasing confidence in its conclusions.
- Systematic Reviews and Meta-Analyses (Apex): These synthesize and statistically aggregate the findings from multiple high-quality primary studies on a specific question. They sit at the peak because they offer the most comprehensive and least biased estimate of an effect. They are, in essence, the distillation of current collective knowledge
- Randomized Controlled Trials (RCTs): Considered the gold standard for establishing cause-and-effect relationships (especially in clinical settings), RCTs randomly assign participants to an intervention group or a control group. This randomization helps to ensure that any observed differences in outcomes are due to the intervention itself, not pre-existing differences between the groups
- Cohort Studies: These longitudinal studies follow groups of people (cohorts) over time to see who develops a specific outcome, comparing those who were exposed to a risk factor versus those who were not. They are crucial for studying prognosis and causation when randomization is unethical or impractical (Epidemiology)
- Case-Control Studies: These retrospective studies compare individuals who have a condition (cases) with those who do not (controls), looking back in time to identify differences in past exposures or risk factors. They are particularly useful for rare diseases
- Case Series and Expert Opinion (Base): These are observational accounts of a few patients or the unverified belief of an authority figure. While they can generate hypotheses, they lack controls and internal validity, placing them at the foundation of the hierarchy and requiring significant skepticism before application
Component II
Professional Expertise and Experience
External evidence provides general guidance, but effective application relies critically on the internal, practical knowledge accumulated by the practitioner over years of work. This component encompasses the clinical or professional skills, judgment and experience that a competent professional has developed through continuous learning and reflective practice.
- Pattern Recognition and Tacit Knowledge: This involves the ability to recognize complex situations and subtle cues—the "art" of the profession—which often cannot be fully codified in research protocols. For example, a seasoned teacher can instinctively identify when a student's lack of engagement is due to a learning difficulty versus an emotional barrier (Education)
- Resource Allocation and Contextualization: Expertise includes understanding the practical constraints of the working environment—budget limitations, organizational culture, staffing levels or system rigidities—and skillfully tailoring an evidence-based intervention to fit these real-world conditions without compromising its core efficacy
- Diagnostic and Prognostic Acumen: The ability to quickly and accurately assess an individual's specific issue, forecast likely outcomes based on that assessment and monitor the individual's response to an intervention, making necessary, real-time adjustments
Component III
Client Values, Preferences and Circumstances
The third, non-negotiable component ensures that EBP remains human-centered and contextualized. It recognizes that even the most robust scientific evidence must be filtered through the unique lens of the person or organization receiving the intervention. Factors for Individualized Application include:
- Personal Preferences and Autonomy: Individuals have a right to choose interventions that align with their personal beliefs, comfort levels and priorities. For instance, a manager implementing an evidence-based organizational change program must consider the team's inherent aversion to a new software tool, even if the research proves its efficiency (Management)
- Unique Circumstances and Social Context: The evidence may suggest a general best practice, but the client's specific life situation, cultural background, economic status and support system drastically affect feasibility and compliance. An intervention requiring daily time commitment may be infeasible for a single parent working three jobs
- Therapeutic Alliance/Relationship Building: For an intervention to be successful, there must be mutual respect and agreement between the professional and the client. A practice that is highly effective in a laboratory setting will fail if the client does not trust the professional or perceive the intervention as relevant to their personal goals
The EBP Process
Implementing EBP is not a passive act of information consumption; it is a five-step, dynamic problem-solving cycle:
- Formulating an Answerable Question: The complex problem must be distilled into a focused, searchable question. In clinical settings, this often follows the PICO format: Patient/Population, Intervention, Comparison, Outcome. For a business context, it might be the PICOC format, adding Context
- Searching for the Best Evidence: The practitioner systematically and efficiently locates the highest-quality, most relevant research to answer the formulated question, often utilizing specialized databases and search strategies
- Critically Appraising the Evidence: This is the most intellectual demanding step. It involves scrutinizing the research for validity (was the study conducted rigorously?), reliability (are the results consistent?) and applicability (can these findings be used in this context?) The professional must be skilled at detecting methodological flaws and bias
- Integrating Evidence with Expertise and Values: The critically appraised external evidence is combined with the practitioner's developed expertise and adapted to fit the client's particular circumstances and preferences, leading to a consensus on the best course of action
- Evaluating Outcomes: After implementation, the results of the decision are rigorously monitored and measured. This crucial step closes the loop, providing new, direct evidence that feeds back into the practitioner's personal experience and informs future practice modifications. This continuous feedback mechanism ensures EBP is a self-correcting system
Critical Appraisal Of the EBP Process
Critical appraisal is the systematic process of judging the trustworthiness, relevance and meaning of published research. It acts as the necessary filter between the vast ocean of scientific literature and the specific needs of the professional decision. A practitioner cannot simply assume a study's conclusion is correct because it is published; they must actively interrogate its methodology.
Three Core Questions of Critical Appraisal
When assessing a piece of research, particularly an intervention study like a Randomized Controlled Trial, the practitioner must address three fundamental categories of inquiry:
- Question 1: Validity (Trustworthiness): Did the study design and execution minimize the chance of bias? This relates to the internal rigor. Key checks include looking for proper randomization methods, the use of blinding (single, double or triple), clear definitions of the intervention and control groups and accounting for all participants who entered the trial (e.g., assessing attrition bias)
- Question 2: Results (Meaning): What were the outcomes and how precise are they? This involves understanding the numerical findings. Practitioners must move beyond binary "statistically significant" conclusions and examine the actual magnitude of the effect (the effect size) and the certainty around that estimate, often measured by the Confidence Interval (CI). A narrow CI suggests high precision in the finding
- Question 3: Applicability (Relevance): Can these results be applied to my client or context? The study might be flawless, but irrelevant. The professional must assess if the study population is sufficiently similar to their client population, if the intervention is feasible in their setting (e.g., too expensive, too complex) and if the benefits outweigh the potential harms given the client's values (Component III)
If the research fails the validity check, it must be discarded, as the results are likely misleading. If it passes validity but fails the relevance test, the evidence, though true, cannot guide the current decision. The critical appraisal process transforms the consumer of information into a discerning gatekeeper of knowledge.
Developing Focused PICO Questions
The initial step of EBP, formulating a focused, searchable question, is pivotal. If the question is too broad ("What treatments exist for depression?"), the literature search will yield thousands of irrelevant papers. If it is too narrow ("Does 10mg of Sertraline cure depression in 47-year-old left-handed men?"), the search may yield nothing. The PICOframework provides the necessary structure to create the Goldilocks Question—one that is just right for efficient searching and relevant evidence gathering.
- P – Patient/Population/Problem: Define the group or individual of interest. Example: Adult hospital patients with acute delirium
- I – Intervention/Exposure: Define the treatment, policy, program or exposure being considered. Example: Scheduled therapeutic recreation activities
- C – Comparison: Define the main alternative to the intervention (this is often standard care or placebo). Example: Standard care (no scheduled therapeutic recreation)
- O – Outcome: Define the measurable result you are trying to affect. Example: Reduction in length of hospital stay
The structured question then becomes: "In adult hospital patients with acute delirium (P), does implementing scheduled therapeutic recreation activities (I) compared to providing standard care (C) result in a reduction in the length of hospital stay (O)?" This precise formulation allows the practitioner to use the PICO elements as highly effective keywords for searching biomedical and health management databases.
Case Study: Pfizer's Vaccine Development
The accelerated development and deployment of the BNT162b2 COVID-19 vaccine by Pfizer (a publicly traded company) in partnership with BioNTech stands as a powerful, large-scale demonstration of Evidence-based Practice in action, particularly focusing on the rapid generation and application of high-quality External Scientific Evidence (Component I).
The Challenge
In early 2020, the world faced a novel pandemic requiring an unprecedented biomedical intervention. The decision to invest billions and mobilize global resources into a new technology—messenger RNA (mRNA)—was based on preliminary, yet compelling, decades-long fundamental research, not traditional vaccine science. The question was: could this lab-scale evidence be rapidly translated into a safe and effective, mass-producible human intervention?
EBP in Action
- The Question: Is the mRNA vaccine BNT162b2 safe and effective at preventing symptomatic COVID-19 infection in diverse adult populations? (PICO: Population = Diverse adults; Intervention = BNT162b2; Comparison = Placebo; Outcome = Prevention of symptomatic disease)
- Generating the Evidence (Component I): Pfizer and BioNTech executed one of the largest and fastest Randomized Controlled Trials (RCTs) in history. This trial involved approximately 44,000 participants globally. Critically, the study was double-blinded, meaning neither the participants nor the researchers knew who received the vaccine and who received the saline placebo, maximizing internal validity and minimizing observation bias. This RCT provided the definitive, gold-standard evidence needed for regulatory approval and global deployment
- Expertise Integration (Component II): Pfizer's internal professional expertise—spanning logistical supply chain management, complex chemistry, manufacturing controls and large-scale clinical trial execution—was paramount. Evidence of efficacy from the RCT needed to be married with the logistical expertise to manage an ultra-cold chain distribution system, ensuring the delicate mRNA product remained viable from the factory floor to the injection site. This required novel, expert-driven solutions that went beyond the RCT data alone
- Client/Societal Values (Component III): The intervention's application was filtered through governmental and societal values for speed and access. Regulators like the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) created a framework for "Emergency Use Authorization" (EUA). This decision recognized the overwhelming societal preference for an immediate, effective intervention to save lives (the value/circumstance), outweighing the traditional, multi-year wait for full licensure, provided the initial RCT data (the evidence) was overwhelmingly positive
- Evaluation: Post-deployment pharmacovigilance (real-world surveillance) continued, confirming the high efficacy rates observed in the initial RCTs and detecting rare side effects (e.g., myocarditis), which allowed medical professionals to refine their treatment and communication protocols (closing the EBP loop)
The Pfizer case is a textbook example of how the methodical application of the most rigorous research (the RCT), integrated with profound professional expertise (ultra-cold chain logistics, large-scale manufacturing) and balanced against unique societal values and circumstances (global pandemic, need for speed), leads to an evidence-based intervention with global impact.
Application in Organizational Psychology
The principles of Evidence-based Practice are equally transformative in organizational psychology (Organizational Psychology) and Human Resource (HR) management, where intuition often dominates decisions about hiring, training and leadership.
The Challenge of Intuitive HR Decisions
Managers frequently rely on gut feeling, inherited company practices or faddish consulting advice when making critical human capital decisions. For instance, the traditional job interview, despite being widely used, is demonstrably a poor predictor of future job performance. A decision to hire based predominantly on an interviewer's subjective impression is a decision made without strong external evidence.
EBP Applied to Talent Acquisition
- The Question: What is the most reliable and valid way to predict the future job performance of candidates for a specialized technical role?
- Searching and Appraising the Evidence (Component I): An HR professional trained in EBP would search the literature for systematic reviews on the predictive validity of various selection methods. The external evidence consistently points to Cognitive Ability Tests and Structured Behavioral Interviews as having the highest correlation with subsequent job success (Personnel Psychology). The lowest predictive validity is generally found in unstructured interviews and personality tests administered in isolation
- Expertise Integration (Component II): The HR expert recognizes that while a cognitive test is predictive, it might face resistance within the organizational culture or legal constraints in the specific jurisdiction. The expert utilizes their deep knowledge of the company's technical requirements to design a structured interview that asks job-relevant, standardized questions and trains hiring managers to use a calibrated scoring rubric, ensuring consistent application across all candidates. This tailors the evidence to the context
- Client/Candidate Values (Component III): The team decides to integrate a realistic job preview video into the process. While not the most powerful predictor, the evidence suggests job previews increase candidate self-selection and satisfaction, thereby respecting the candidate's value for transparency and reducing eventual turnover. The overall process respects fairness and candidate experience, adapting the evidence-based selection tools to fit the values of a positive organizational image
- Evaluation: Six months after implementation, the organization tracks the job performance ratings and turnover rates of the new hires who went through the revised, evidence-based process versus legacy hires. Data demonstrating a clear reduction in turnover and an increase in average performance metrics confirms the utility of the EBP application
This shift moves HR away from a purely administrative function to a strategic discipline, utilizing quantifiable evidence to improve organizational effectiveness and demonstrate a measurable return on investment for human capital initiatives.
Evidence-based Practice (EBP) is a non-negotiable methodology for contemporary professional disciplines, establishing a framework that elevates rational decision-making above unexamined tradition or mere personal authority. It operates on the principle of integrating the three essential elements: the highest quality scientific research, the seasoned professional's accumulated expertise and practical wisdom and the specific, unique values and circumstances of the person or entity being served. The process is a continuous, five-step cycle beginning with asking a focused question and concluding with evaluating the implemented outcome, thereby constantly refining practice. By demanding that professionals actively seek, critically evaluate and judiciously apply data, EBP ensures decisions are transparent, justifiable and optimized for achieving verifiable, positive results in any complex, knowledge-driven domain
Citation
Cite this article
Sridharan, M. A. (2024, December 12). Evidence-based Practice (EBP). Think Insights. https://thinkinsights.net/consulting/evidence-based-practice-ebp (Accessed [[ACCESS_DATE]])
Sridharan, Mithun A. "Evidence-based Practice (EBP)." Think Insights, 12 Dec. 2024, https://thinkinsights.net/consulting/evidence-based-practice-ebp. Accessed [[ACCESS_DATE]].
Mithun A. Sridharan, "Evidence-based Practice (EBP)," Think Insights, December 12, 2024, https://thinkinsights.net/consulting/evidence-based-practice-ebp. Accessed [[ACCESS_DATE]].
Sridharan, M.A. (2024) 'Evidence-based Practice (EBP)', Think Insights. Available at: https://thinkinsights.net/consulting/evidence-based-practice-ebp (Accessed: [[ACCESS_DATE]]).
M. A. Sridharan, "Evidence-based Practice (EBP)," Think Insights, 2024. [Online]. Available: https://thinkinsights.net/consulting/evidence-based-practice-ebp. [Accessed: [[ACCESS_DATE]]].
Sridharan MA. Evidence-based Practice (EBP). Think Insights. Published December 12, 2024. Accessed [[ACCESS_DATE]]. https://thinkinsights.net/consulting/evidence-based-practice-ebp
Test Your Knowledge
Evidence-based Practice (EBP)
Challenge yourself on the concepts from this article and see how well you understood them.
Subscribers get weekly quizzes and insights — subscribe free
Sponsor this article
Partner with Think Insights
Reach 50,000+ business leaders, consultants, and strategists. Feature your brand alongside expert articles on strategy, leadership, and digital transformation.
Become a Sponsor